Concern about abnormal head shape in
infants is common. Infants born prematurely are at higher risk for cranial
deformation (often dubbed “positional plagiocephaly”) than those born at term,
though it occurs in about 20% of the latter and has become more common since the
American Academy of Pediatrics instituted the “Back to Sleep” campaign in 1994.
[Rogers: 2011]
[Rogers: 2011]
[Task: 2000]
Cranial deformation occurs in response to external forces either in utero or after
birth, and sutures close normally. Craniosynostosis, involving premature closure of
1 or more of the cranial sutures, is far less common for both preterm and term
infants but can look similar to some deformational abnormalities. Craniosynostosis
is estimated to occur in 1:2500 infants. It is thought to be caused by combinations
of genetics, bone, and epigenetic factors, with a small subset linked to a genetic
syndrome. Maternal thyroid disease during pregnancy or prenatal use of clomiphene
citrate, a fertility medication, is associated with increased risk of
craniosynostosis. In addition to being sensitive to aesthetic concerns related to
abnormal head shape, primary care clinicians need to be vigilant for abnormal brain
growth and intellectual development that can occur with craniosynostosis.
ICD-10 Coding
Q 67.3, Plagiocephaly (can result from either craniosynostosis or external forces
[nonsynostotic plagiocephaly])
Early referral of craniosynostosis is critical Most of these are evident at birth or within the first 2-3 weeks of
life after swelling from birth subsides. Positional deformities usually become
increasingly evident in the weeks and months after birth and may have a normal
appearance at birth.
Timing of anterior fontanelle closure Be aware that 10% close by 3 months, 90% by 18 months. “If the shape
is normal, ignore the fontanelle.” [Kestle: 2020] This
means you do not need to refer for evaluation of early fontanelle closure unless
head shape is abnormal. Consider evaluation for hyperthyroidism,
hyperparathyroidism, hypophosphatasia, or rickets, as these can be associated with
early fontanelle closure. [Dias: 2020]
Ridged sutures If the overall shape is normal, but there are ridges on the sutures,
then no referral is needed.
Imaging Radiographs are not advised. Consultation with pediatric plastic
surgery and/or pediatric neurosurgery prior to ordering CT imaging is
prudent.
Prevention of deformation Provide anticipatory guidance to parents of newborns about how to
prevent deformation. In addition to routine safe sleep recommendations, encourage
positioning the infant’s head to alternating sides during sleep. Stimulate the baby
from all directions by arranging toys around the infant and approaching the infant
from different sides. Encourage “tummy time” when awake and avoid extended time in
bouncers and car seats.
Microcephaly Defined as a head circumference <5%ile for age, microcephaly is
almost never caused by craniosynostosis of a single suture but can occur in complex
craniosynostosis. [Dias: 2020]
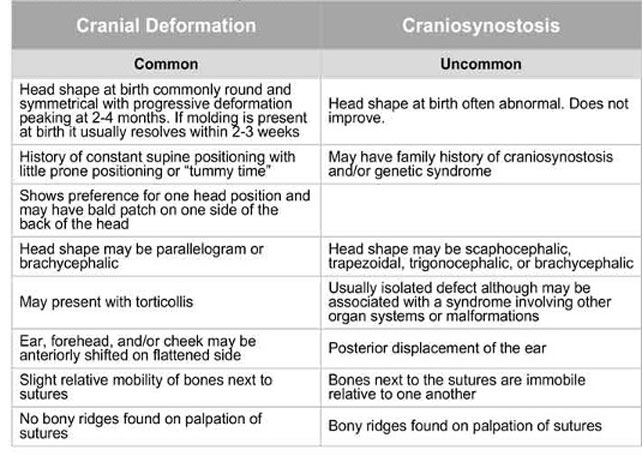
Differentiating Deformation from Synostosis
Differentiating craniosynostosis from deformational abnormalities requires a
thorough history and physical of the infant. It also may require imaging. Since many
infants will have deformational cranial abnormalities, the decision to image the
infant using head computerized tomography (CT) may be best left to the specialist,
perhaps reducing needless radiation exposure. [Siddiqi: 2020]
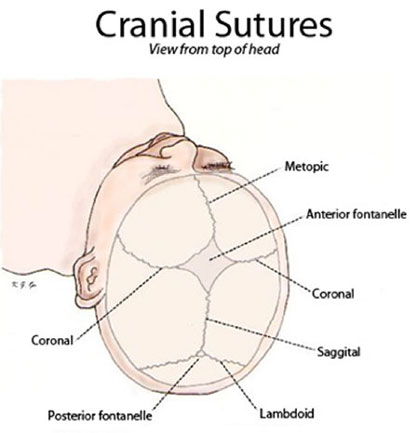
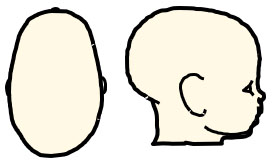
Normal Head Shape with Sutures
Differentiating Craniosynostosis from Deformational Abnormalities
Deformation of the head shape is quite common in infants, present in 20-50% of
6-month olds. [Dias: 2020] Flattening occurs when cranial
expansion and growth are consistently resisted in one area of the skull by an
external force. [Rogers: 2011]
[Rogers: 2011] Limited independent head mobility in very
young infants or those with congenital muscular torticollis contribute to the
flattening. Growth of the cranium is most rapid in the first few months of life, and
treatment is most effective in that time frame. Premature infants have more limited
head mobility for longer than full-term infants, which may explain their higher
frequency of deformational cranial abnormalities. This brief video reviews how to
evaluate for torticollis: Torticollis Quick Screening Guide by Lisa Hwang, DPT, Dsc Candidate.
Also see, Premature Infant Follow-Up
Cranial deformation takes several forms.
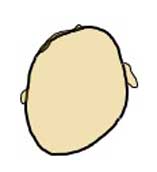
Deformational Plagiocephaly
Deformational PlagiocephalyDeformational plagiocephaly, or positional plagiocephaly, is
the flattening of one side of the posterior skull, creating an oblique or
slanted head when viewed from the top. Ipsilateral (along the same side) frontal
bossing and asymmetric facial features result; however, the degree of flattening
of the occipital skull is more pronounced and results in a parallelogram shape
when viewed from above the infant’s head. The ear may be positioned more
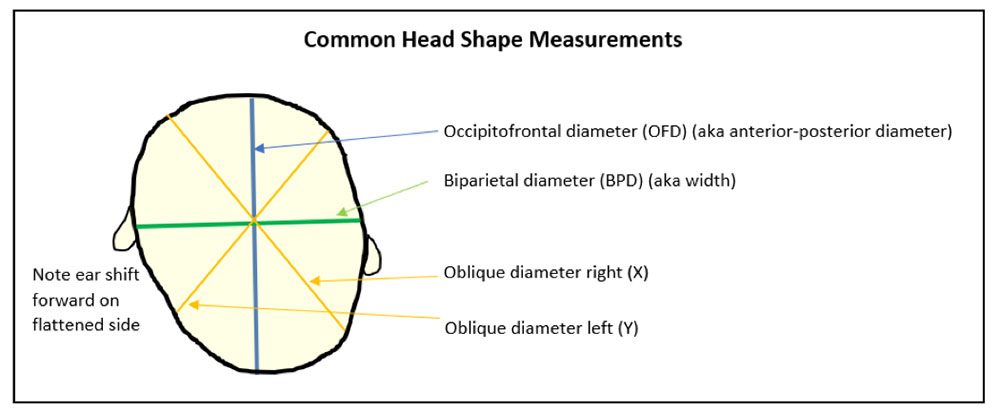
anteriorly on the side of the flattening.
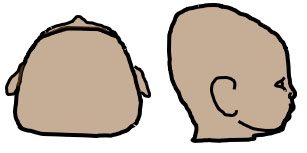
Deformational Brachycephaly
Deformational BrachycephalyDeformational brachycephaly is the symmetric flattening of
the occipital skull with compensatory bi-parietal widening, giving the
appearance of a large head when viewed from the front. Some degree of asymmetry
is commonly seen. These infants may also have a posterior protrusion at the top
of the head. When looking at the infant skull from the side, the skull appears
to slope downward towards the anterior portion of the head. This is called
“turricephaly” or a “tall head.” There can be a combination of deformational
brachycephaly and plagiocephaly, resulting in some asymmetry.
Deformational Scaphocephaly
Deformational ScaphocephalyDeformational scaphocephaly (also known as dolichocephaly or
“NICUcephaly”) is an uncommon variant with an elongated head shape without
biparietal narrowing. This is most often seen in preterm infants who have been
positioned on their sides, resulting in flattening of the sides of the head and
compensatory increase in the anterior posterior dimension of the cranium.
Preventive measures instituted in NICUs have decreased the incidence of
this.
Anthropomorphic measurements can be obtained. There are age-matched
normative values for the cephalic index (CI), which is the maximum width of the
head divided by the anteroposterior length, and the plagiocephaly index, which
compares the differences between the 2 oblique diameters. However, the
interpretation of normal is culturally based and may not affect the decision to
treat. The author, Rogers, suggests the strongest indication to treat is the
parent’s opinion of deformity. [Rogers: 2011]
[Rogers: 2011]
Cephalic Index = BPD/OFD x 100
Normocephalic or plagiocephaly: 76-90%
Brachycephaly: >90%
Dolichocephaly: <76%
Plagiocephaly Index (aka Oblique Diameter Difference) = [X – Y]
(in mm)
Normal: 0-4 mm
Mild: 5-9 mm
Moderate: 10-15 mm
Severe: >15 mm
Management of Cranial Deformation
Treatment for positional deformation is repositioning and helmets. Evidence does
not support the use of helmets in moderate-severely affected infants ages 5-6
months. A 2016 randomized controlled trial observed equal improvements in head shape
in follow-up of infants who were helmeted vs. natural course; however, the study
excluded premature infants <35 weeks and those with torticollis or other
deformities. [van: 2014] Helmets may not be covered by
insurance; coverage improves if there is also torticollis. Based on the timing of
fontanelle closures, helmeting is most likely to be effective if initiated by 4
months of age, but it may not improve outcomes.
Mechanical adjustments and exercises: These can be done
at home. They include positioning the infant’s rounded side of the head
against the mattress and changing the crib’s position so the infant would
need to look away from the flattened side to see people enter the room.
[Laughlin: 2011]
[Morris: 2016] Some specialists advise placing a
wedge or rolled up blanket under the torso on 1 side to appropriately
position the child. Repositioning only works prior to the infant acquiring
independent head control, which typically occurs by 4 months of age,
corrected. Within 2-3 months, most infants will show improvement.
[Task: 2000] This brief video demonstrates
holding positions for parents to help stretch the baby’s neck muscles:
Torticollis Holding Positions -COA PTOT.
Physical therapy addresses congenital muscular
torticollis (CMT) and positional preferences. A physical therapist can teach
parents to address congenital muscular torticollis (CMT) and positional
preferences with 3 repetitions of stretches performed several times daily,
such as at each diaper change. [Laughlin: 2011] The
stretches usually involve placing one hand on the child’s upper chest while
the other gently moves the chin until it touches the shoulder. This is held
for 10 seconds and then repeated for the other side. [Laughlin: 2011] This short video demonstrates exercises that parents
can do at home to augment physical therapy for torticollis: How to Treat Torticollis - DadLabs Video.
Consider referral to a pediatric neurosurgeon or plastic surgeon or to a
craniofacial specialist if improvement does not improve by 4 months of age.
Treatments that might then be considered are: [Laughlin: 2011]
Sleep orthotic or cradle devices position the infant’s
occiput on a concave rather than a flat surface. This redistributes the
surface pressure on the occiput but maintains the infant in the supine
position. This approach only works prior to 3-4 months of age corrected,
when infants develop sufficient head control to defeat its purpose.
Helmet therapyHelmet therapy is an orthotic that is typically used for
moderate to severe deformational flattening. [Rogers: 2011]
[Rogers: 2011] Several principles are important:
Helmets would only have the potential to be
effective when there is remaining skull growth.
Younger children correct quicker than older
children, consistent with the rate of growth of the cranium.
Helmets do not apply pressure to the cranium but
rather have foam selectively cut away from the area in which growth
is desired. They do not mold or squeeze the cranium.
A skilled orthotist is needed to monitor the growth
of the infant’s head and the fit of the helmet.
Prevention includes:
Preventive counseling by 4 weeks of age: Provide
information about tummy time while the infant is awake and observed (at
least 30-60 minutes) and alternating head position at night during sleep.
Encourage full, symmetric, unrestricted movements while awake. [Morris: 2016] Too much time in safety seats or swings
should be discouraged. [Rogers: 2011]
Evaluation of Craniosynostosis
Head shape is dependent on which sutures are fused.
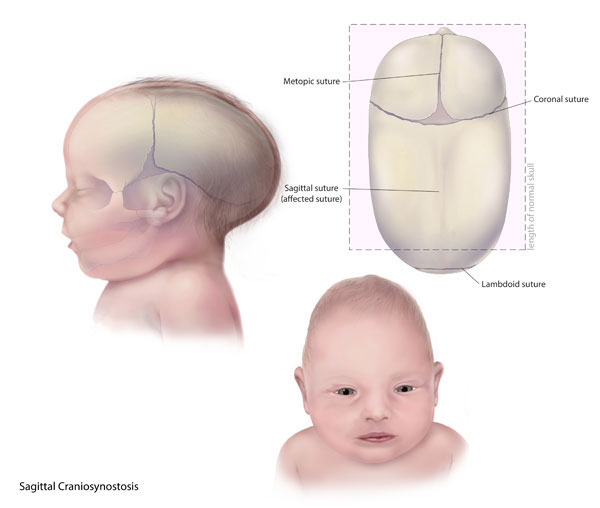
Sagittal synostosis is the most common type of craniosynostosis,
occurring in 2-3.2 per 10,000 live births and occurs more commonly in males.
[Dias: 2020] Early closure of the suture running along
the top of the head results in an elongated head shape (scaphocephaly) and
biparietal narrowing, which can appear bullet-shaped posteriorly and downward
sloping. Frontal or occipital bossing may occur, and a sagittal ridge may be
palpated. A saddle deformity may be present at the vertex when viewed from the side.
Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities
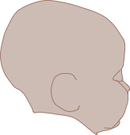
BathrocephalyThe primary care clinician should differentiate sagittal synostosis from
dolicocephaly (see Deformational Scaphocephaly, above) and
from bathrocephaly (associated with a persistent mendosal suture
(a suture that runs transversely between the lambdoid sutures that usually closes in
utero), presenting with a prominent occiput with sharp angulation toward the neck
but without frontal bossing, biparietal narrowing, or a sagittal ridge).
Bathrocephaly does not require intervention.
Metopic synostosisMetopic synostosis with trigonocephaly is the second
most common type of craniosynostosis, occurring in 0.9-2.3 per 10,000 live births,
and affects more males than females. [Dias: 2020] Metopic
synostosis develops due to early fusion of the metopic suture, which runs from the
top of the nose mid-forehead to the sagittal suture, leading to a trigonocephalic or
triangular shape with a mid-forehead prominence. Hypotelorism may be present. Less
severe “mild trigonocephaly” with mildly wider back compared to front of the head
may not require surgical intervention. A ridge over the metopic suture without
trigonocephaly does not require imaging or surgical intervention.
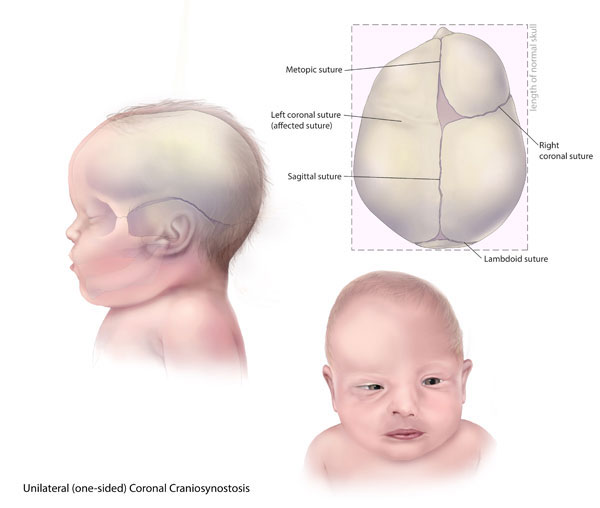
Unioronal synostosis is when one of the coronal sutures
running from the ear to the sagittal bone closes early, and anterior plagiocephaly
develops on the side of the early closure. When coronal synostosis occurs, the
contralateral frontal bone protrudes, orbits appear asymmetric, and the eye on the
affected side appears more open (“Harlequin eye”). The bony part of the nose may be
pulled toward the fused suture, and the nasal tip may deviate away from
it.
Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities
Infant with Crouzon syndrome
KateVUk/Wikimedia (CC BY-SA 4.0)
Bilateral coronal synostosisBicoronal synostosis (aka anterior brachycephaly) results in
turribrachycephaly with a broad, tall appearance to the head, a flattened forehead,
and bilaterally palpable coronal sutures. This can lead to exophthalmos and shallow
eye orbits and a shortened nasal bone, and vision problems can occur. Bicoronal
synostosis is more common in syndromic conditions that present with other atypical
physical findings likely to be present, e.g., Crouzon, Apert, and Pfeiffer
syndromes.
Lambdoid synostosisLambdoid synostosis, the rarest type of synostosis, occurs in the
lambdoid sutures at the back of the head. Early closure of one of these results in
flattening on the back on the ipsilateral side, and the ear on that side may be
pulled back or down. A mastoid bony bulge may be present on the affected side. The
forehead will likely appear normal. It may appear trapezoidal when viewed from the
back.
Complex synostosis involves multiple sutures and is quite rare
and more likely associated with a syndrome.
Radiographs are not advised. A CT may be performed to best evaluate suture
abnormalities. Low-radiation CT imaging protocols are gaining traction to
greatly reduce the risk of developing head cancers later in life. Consultation
with pediatric plastic surgery and/or pediatric neurosurgery prior to ordering
imaging is prudent. [Siddiqi: 2020]
Management of Craniosynostosis
Once swelling from birth has subsided in the first week or 2 of life, most cases of
synostosis are readily identifiable. Early referral to pediatric plastic
surgery or pediatric neurosurgery within the first month of life is
advised. In some centers, a synostosis clinic may be available.
Pediatric neurosurgery and pediatric plastic surgery often collaborate on care for
these infants. Contacting the specialists with photos or via video may be useful as
well. [Siddiqi: 2020]
When surgery is indicated, operating as early as 2-3 months of age
(endoscopic-assisted strip craniectomy) may be recommended; however, the actual
timing of surgery will vary depending on which suture is affected, the age at
presentation, and the recommended treatment plan. [Naran: 2017] Open cranial vault surgery by 9-12 months is optimal due to the
relative plasticity of the cranial vault that hardens significantly by 15 months of
age. The expert recommendation for early surgical intervention is based on limited
evidence; later surgical intervention has not been shown to improve outcomes, and
complications are lowest in the earlier surgery groups. Earlier surgical
interventions are associated with better neurodevelopmental outcomes, shorter
operative times, shorter hospitalizations, reduced blood loss, and reduced swelling.
[Mandela: 2019]
[Bellew: 2019]
Treatment promotes a more typical head shape to protect the development of the
orbits, provide adequate space for brain growth, and manage intracranial pressure.
[Morris: 2016] Multiple studies have investigated the
impact of abnormal head shape on children’s emotional well-being; however, there is
a lack of high-quality evidence regarding this outcome. [Chummun: 2016] Elevated ICP is present in about 14-24% of children with
isolated synostosis and can correlate with lower developmental outcomes; if multiple
sutures are present, the risk increases. [Naran: 2017]
However, evidence is unclear whether neurodevelopmental and cognitive outcomes
reliably improve with earlier treatment of craniosynostosis. [Dias: 2020]
With the endoscopic-assisted strip craniectomy approach, serial helmeting is
performed postoperatively for 6-12 months. Continue to monitor children
postoperatively for symptoms and signs of increased ICP, developmental or behavioral
concerns. Provide routine monitoring for problems with dentition, hearing, or vision
and refer as indicated. Follow up within a multidisciplinary craniosynostosis
program is advised, when available. [Siddiqi: 2020]
These specialists also often work together to manage head shape problems
in babies:
Orthotist: A person skilled in providing supportive equipment for
a desired functional outcome. In the case of cranial deformation abnormalities, this
individual makes the helmet and closely monitors its function throughout its use on
the infant’s head to ensure the best growth and prevent skin sores and discomfort
for the infant.
Pediatric Neurosurgery: Provide evaluations, recommendations, and
management for nervous system problems and severe or persistent cranial
deformations. Pediatric Neurosurgery
(see NW providers
[1]).
Craniosynostosis and Positional Plagiocephaly Support (CAPPS) CAPPS — which stands for Craniosynostosis and Positional Plagiocephaly Support — is the pioneer and leader in supporting and
educating families diagnosed with Craniosynostosis and/or Positional Plagiocephaly. The site includes a provider directory.
Practice Guidelines
Dias MS, Samson T, Rizk EB, Governale LS, Richtsmeier JT. Identifying the Misshapen Head: Craniosynostosis and Related Disorders. Pediatrics.
2020;146(3).
PubMed abstract The purpose of this clinical report is to review the characteristic head shape changes, as well as secondary craniofacial
characteristics, that occur in the setting of the various primary craniosynostoses and deformations. The intent is to improve
pediatric care providers’ recognition and timely referral for craniosynostosis and their differentiation of synostotic from
deformational and other nonoperative head shape changes; American Academy of Pediatrics.
* number of provider listings may vary by how states categorize services, whether providers are listed by organization
or individual, how services are organized in the state, and other factors; Nationwide (NW) providers are generally limited
to web-based services, provider locator services, and organizations that serve children from across the nation.
Authors & Reviewers
Initial publication: May 2020; last update/revision: October 2020
Bellew M, Mandela RJ, Chumas PD. Impact of age at surgery on neurodevelopmental outcomes in sagittal synostosis. J Neurosurg Pediatr.
2019:1-8.
PubMed abstract A study of whether age at surgery has an impact on later neurodevelopmental outcomes for children with sagittal synostosis
Chummun S, McLean NR, Flapper WJ, David DJ. The Management of Nonsyndromic, Isolated Sagittal Synostosis. J Craniofac Surg.
2016;27(2):299-304.
PubMed abstract This systematic review assessed cranial index and neuropsychological outcome following surgery for isolated, nonsyndromic
sagittal synostosis.
Dias MS, Samson T, Rizk EB, Governale LS, Richtsmeier JT. Identifying the Misshapen Head: Craniosynostosis and Related Disorders. Pediatrics.
2020;146(3).
PubMed abstract The purpose of this clinical report is to review the characteristic head shape changes, as well as secondary craniofacial
characteristics, that occur in the setting of the various primary craniosynostoses and deformations. The intent is to improve
pediatric care providers’ recognition and timely referral for craniosynostosis and their differentiation of synostotic from
deformational and other nonoperative head shape changes; American Academy of Pediatrics.
Kestle J. ECHO presentation. 2020; Dr. John Kestle, ECHO presentation 4/8/2020.
Laughlin J, Luerssen TG, Dias MS. Prevention and management of positional skull deformities in infants. Pediatrics.
2011;128(6):1236-41.
PubMed abstract / Full Text This AAP practice guideline was retired in 2018.
Looman WS, Flannery AB. Evidence-based care of the child with deformational plagiocephaly, Part I: assessment and diagnosis. J Pediatr Health Care.
2012;26(4):242-50; quiz 251-3.
PubMed abstract / Full Text
Mandela R, Bellew M, Chumas P, Nash H. Impact of surgery timing for craniosynostosis on neurodevelopmental outcomes: a systematic review. J Neurosurg Pediatr.
2019;23(4):442-454.
PubMed abstract This systematic review summarizes and assesses evidence on whether there is an optimal age for surgery in terms of neurodevelopmental
outcomes.
Morris LM. Nonsyndromic Craniosynostosis and Deformational Head Shape Disorders. Facial Plast Surg Clin North Am.
2016;24(4):517-530.
PubMed abstract This article provides an overview of etiology, epidemiology, pathology, diagnosis, and treatment of nonsyndromic craniosynostosis,
indications for surgical intervention and management options. Deformational plagiocephaly is also presented with treatment
options including repositioning, physical therapy, and helmet therapy.
Naran S, Miller M, Shakir S, Ware B, Camison L, Ford M, Goldstein J, Losee JE. Nonsyndromic Craniosynostosis and Associated Abnormal Speech and Language Development. Plast Reconstr Surg.
2017;140(1):62e-69e.
PubMed abstract The article details language acquisition and speech development in children with nonsyndromic craniosynostosis.
Nield LS, Brunner MD, Kamat D. The infant with a misshapen head. Clin Pediatr (Phila).
2007;46(4):292-8.
PubMed abstract
Rogers GF. Deformational plagiocephaly, brachycephaly, and scaphocephaly. Part I: terminology, diagnosis, and etiopathogenesis. J Craniofac Surg.
2011;22(1):9-16.
PubMed abstract
Rogers GF. Deformational plagiocephaly, brachycephaly, and scaphocephaly. Part II: prevention and treatment. J Craniofac Surg.
2011;22(1):17-23.
PubMed abstract
Task Force on Infant Sleep Position and Sudden Infant Death Syndrome. Changing concepts of sudden infant death syndrome: implications for infant sleeping environment and sleep position. American
Academy of Pediatrics. Task Force on Infant Sleep Position and Sudden Infant Death Syndrome. Pediatrics.
2000;105(3 Pt 1):650-6.
PubMed abstract / Full Text
Ursitti F, Fadda T, Papetti L, Pagnoni M, Nicita F, Iannetti G, Spalice A. Evaluation and management of nonsyndromic craniosynostosis. Acta Paediatr.
2011;100(9):1185-94.
PubMed abstract / Full Text
van Wijk RM, van Vlimmeren LA, Groothuis-Oudshoorn CG, Van der Ploeg CP, Ijzerman MJ, Boere-Boonekamp MM. Helmet therapy in infants with positional skull deformation: randomised controlled trial. BMJ.
2014;348:g2741.
PubMed abstract / Full Text







 48 KB), Head Circumference-for-Age Percentiles: Girls, Birth to 36 Months (CDC) (
48 KB), Head Circumference-for-Age Percentiles: Girls, Birth to 36 Months (CDC) (